- Oncosoft Closes 14 Billion KRW Series B2 Funding Round
- Exclusive Distribution Agreement Signed with Chile’s 'OPUS Física Médica
SpA' for OncoStudio
- Three-Year OncoStudio Subscription Agreement Signed with Tohoku University Hospital in Japan
- Selected as Lead Agency for the 2026 National Interministerial Medical Device R&D Project
- CEO Jin Seung Kim Receives Yonsei University Startup Award
- KOSRO 2026: Demonstrating Optimized Workflows and Clinical Utility in Radiation Oncology
- [Column]
- News in RadOnc: Target Contouring Guidelines for Breast Cancer Radiation Therapy
|
|
|
❶ Oncosoft Closes 14 Billion KRW Series B2 Funding Round |
|
|
Oncosoft has successfully closed its Series B2 funding round, securing a total of 14 billion KRW. This investment marks a significant business milestone, validating the clinical utility and commercial stability of the company's AI-based medical software solutions within the capital market.
Key institutional investors focused on the value of Oncosoft’s proprietary core technologies and its unique long-term growth potential. The newly secured capital will be strategically allocated to enhance OncoStudio, the company's core AI-powered automated contouring software, and to develop OncoPlan, its particle radiation therapy planning solution. Additionally, the funds will support global clinical trials, accelerate entry into key overseas markets, and recruit R&D talent to strengthen technical capabilities.
OncoPlan is designed as an alternative in the global particle therapy planning market, which is currently led by foreign software. By leveraging sophisticated, in-house algorithms, OncoPlan aims to maximize treatment precision while integrating next-generation AI to streamline complex workflows. With this strengthened financial foundation, Oncosoft intends to solidify its technological position in the medical AI sector and expand its global commercialization efforts. |
|
|
❷ Exclusive Distribution Agreement Signed with Chile’s 'OPUS Física Médica SpA' for OncoStudio |
|
|
As part of its global market diversification strategy, Oncosoft has signed an exclusive distribution agreement for the Chilean market with OPUS Física Médica SpA, a medical device distributor in Latin America.
OncoStudio has obtained medical device clearances in five countries, including South Korea, Japan, the United States, Singapore, and Brazil, demonstrating globally recognized clinical and technical value across diverse healthcare environments. The partnership was driven by OncoStudio’s adoption and reliability in real-world clinical settings across Korea and Japan, both of which maintain strict regulatory standards.
This agreement marks OncoStudio’s first official entry into the South American market. Given that Chile serves as a healthcare hub with advanced medical infrastructure in Latin America, establishing a presence there is highly significant for the company. Oncosoft plans to leverage this agreement to secure local references while expanding into neighboring Latin American markets, building upon its existing clearance in Brazil. |
|
|
❸ Three-Year OncoStudio Subscription Agreement Signed with Tohoku University Hospital in Japan |
|
|
Oncosoft has signed a three-year subscription contract with Tohoku University Hospital in Japan for OncoStudio. This export agreement includes the company's proprietary 'MR Segmentation Model', which will be deployed in alignment with the hospital's clinical schedule.
Securing a long-term subscription contract in Japan—a market with stringent software validation and adoption criteria—is a notable achievement for the company. Through this contract, Oncosoft continues to stabilize its export performance in Japan and maintain revenue growth in overseas markets, aiming to gradually expand its footprint into other major global markets. |
|
|
❹ Selected as Lead Agency for the 2026 National Interministerial Medical Device R&D Project |
|
|
Oncosoft has been selected as the lead agency for the 2026 National Interministerial Medical Device R&D Project and is currently finalizing the project agreement. Under the project titled "Commercialization and Business Development of a Domestic Technology-Based Heavy Ion Carbon Beam Treatment Planning System (TPS)," Oncosoft will serve as the lead agency, collaborating with the Yonsei University Health System as a co-investigator. This initiative runs from April 2026 to December 2028, with a total project budget of 2.7 billion KRW, which includes a 2.2 billion KRW government grant.
Currently, the domestic heavy ion TPS market relies heavily on foreign imports. This project aims to address this reliance by establishing technological self-reliance over heavy ion treatment planning systems and localizing this next-generation cancer treatment software. In line with this initiative, Oncosoft submitted its application for domestic medical device clearance for the heavy ion TPS in April 2026. Through this project, the company aims to establish itself as a global TPS provider while enhancing high-precision medical software capabilities. |
|
|
❺ CEO Jin Seung Kim Receives Yonsei University Startup Award
|
|
|
Oncosoft CEO Jin Seung Kim has received the 'Faculty Startup' Award at the Yonsei University Startup Awards. This award recognizes the research achievements and contributions to commercialization made by CEO Kim, who serves as both a professor in the Department of Radiation Oncology at Yonsei University College of Medicine and the head of Oncosoft.
Oncosoft develops AI-driven radiation therapy technologies, centered around heavy ion therapy, integrating clinical technologies and expertise from the Yonsei University Health System. Driven by these capabilities, the company has secured over 25 billion KRW in cumulative investments to date. Oncosoft remains focused on medical technology development and collaboration with academia through continuous R&D and commercialization. |
|
|
❶ KOSRO 2026: Demonstrating Optimized Workflows and Clinical Utility in Radiation Oncology
|
|
|
Oncosoft participated in the KOSRO 2026 Spring Meeting, hosted by the Korean Society for Radiation Oncology, where the company operated a dedicated exhibition booth. At the symposium, Oncosoft demonstrated the updated clinical workflows of its AI-based radiation therapy solutions and discussed their clinical utility with radiation oncologists and medical professionals. Throughout the exhibition, the company gathered real-world feedback and assessed the practical needs of medical staff.
The insights and suggestions gathered during this symposium will be integrated into upcoming R&D to further enhance product features and clinical applicability. |
|
|
✅ Target Contouring Guidelines for Breast Cancer Radiation Therapy
In Korea, the adoption of IMRT for breast cancer radiation therapy has grown rapidly and has now effectively become the standard of care. Consequently, the workload and complexity dedicated to target contouring have increased significantly compared to the past. While various factors, such as the planning method, influence the outcome, the actual dose delivered to organs at risk (OARs) like the heart and lungs varies significantly depending on the target contouring. Notably, the KROG 19-01 study demonstrated that even for the same patient, the doses to the heart and lungs differ considerably depending on which contouring guideline is applied.
Historically, the RTOG atlas has been widely used in Korea. However, in the mid-2010s, the ESTRO consensus guidelines were published (Offersen B et al. Radiother Oncol 2015;114:3–10). While RTOG is rooted in the concepts of field-based planning using bony landmarks from the 2D era, ESTRO introduced criteria based on blood vessels to align with the era of volume-based planning. Generally, ESTRO defines smaller volumes than RTOG. For instance, the supraclavicular lymph node (SCL) volume is smaller as Level IV, which reduces the radiation dose to the thyroid. The breast volume is also contoured smaller, meaning that doses to normal organs such as the heart, lungs, and thyroid can be further spared. |
|
|
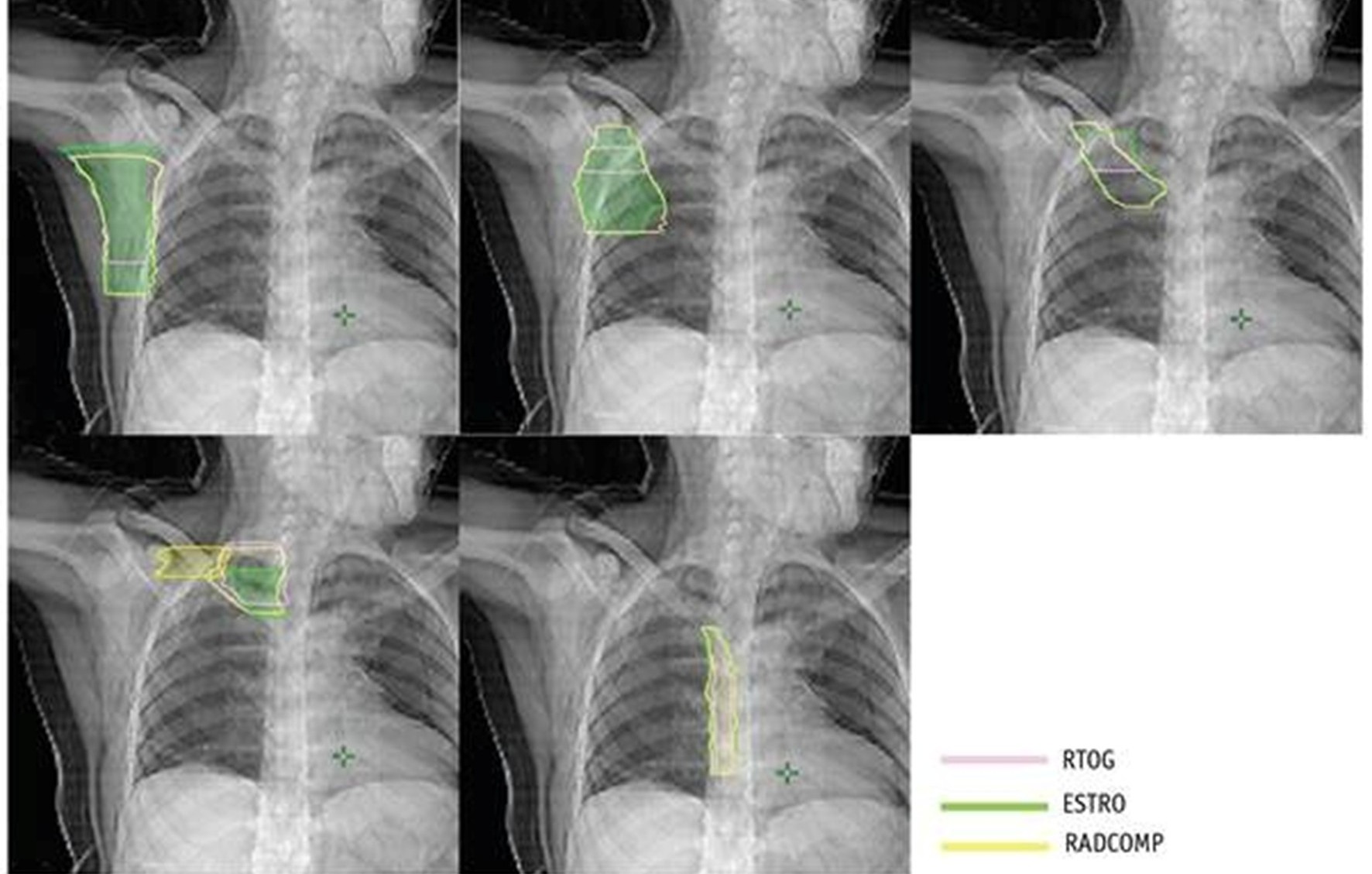
Figure 1. A 2D comparison of axillary node (Level I–IV) and internal mammary node regions defined by three guidelines (RTOG, ESTRO, and RADCOMP). ESTRO generally proposes smaller volumes. (Loganadane G, et al. Int J Radiat Oncol Biol Phys. 2020;107(3):437–448)
|
|
|
However, the adoption of the ESTRO guidelines appears to be slow in both North America and Korea. In North America, many centers still perform field-based planning by contouring only the lymph nodes (LNs) without outlining the breast target. Even when IMRT is occasionally utilized, they still tend to follow the RTOG guidelines, and I am aware that many hospitals in Korea also continue to use RTOG. This is likely due to the concern: “What if contouring a smaller volume leads to a marginal miss?”
To address this concern, I previously conducted retrospective validation studies of the ESTRO guidelines using Yonsei University data (Chang JS et al. Radiother Oncol 2017;122:24–29) and KROG multi-center data (Chang JS et al. Radiother Oncol 2018;126:139–147). The conclusion was that “the vast majority of recurrences are well contained within the ESTRO target,” but these findings were limited by their retrospective nature. Recently, the Danish Breast Cancer Group (DBCG) published validation results from a large-scale prospective study, and today I would like to introduce this paper. |
|
|
✅ Validating ESTRO Through a Prospective Study
|
|
|
The paper introduced here is a pre-planned analysis of the DBCG Skagen Trial 1. The Skagen Trial 1 is a phase III randomized controlled trial comparing loco-regional RT at 40 Gy in 15 fractions (moderate hypofractionation) versus the standard 50 Gy in 25 fractions for high-risk breast cancer. Between 2015 and 2021, 2,963 patients (2,908 in the intention-to-treat [ITT] population) were enrolled across 17 institutions in 7 countries, and the results were presented at ESTRO 2025.
In this study, target contouring strictly adhering to the ESTRO guidelines was mandatory for all cases. Furthermore, all patients with indications for loco-regional RT were eligible for inclusion. Consequently, even patients with a substantial nodal burden were fully represented in the study population.
At a median follow-up of 5.2 years (IQR 4.1–6.7), loco-regional recurrence (LRR) occurred in 78 patients (5-year cumulative LRR risk of 2.7%, 95% CI 2.1–3.4%). Among these, 74 recurrences (95%) occurred inside the ESTRO CTV. Across the entire ITT population of 2,908 patients, clear marginal misses occurred in only 3 patients (of which only 2 cases completely escaped the ESTRO volume itself). What was particularly impressive was that there was only a single recurrence in the areas included in RTOG but excluded from ESTRO—such as the upper SCL extending up to the cricoid or the region medial to CTVn_L4. |
|
|
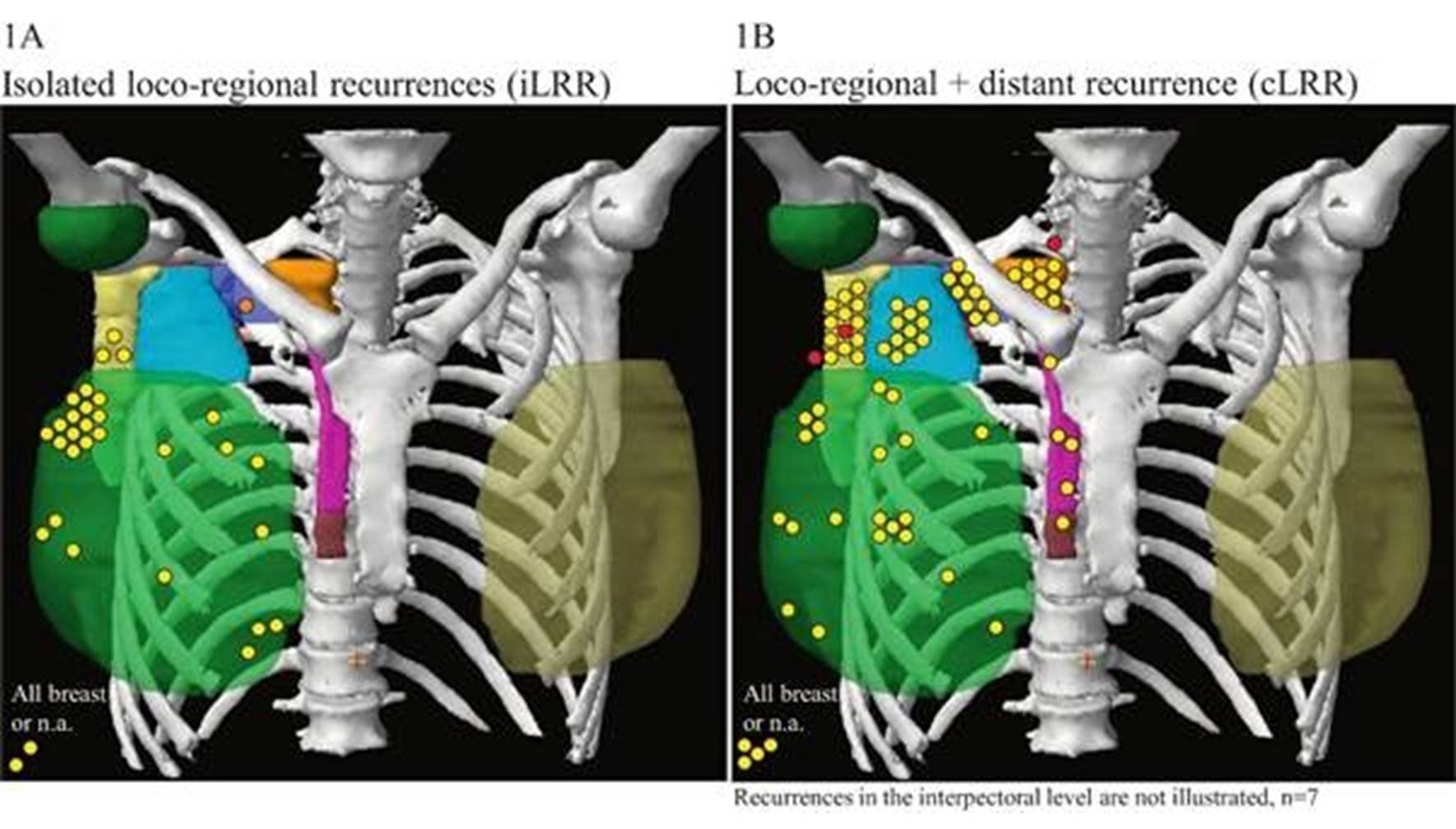
Figure 2. Mapping of loco-regional recurrence (LRR). (A) Isolated LRR (iLRR; n=41). (B) LRR concurrent with distant metastasis (cLRR; n=37). Yellow markers indicate recurrence inside the CTV, orange markers indicate recurrence outside the CTV but within the full prescribed dose area, and red markers represent a marginal miss (50–90% dose). Each marker represents one patient per involved volume. (Høgsbjerg KW, et al. Radiother Oncol 2026, in press)
|
|
|
Who, then, were those few patients who recurred outside the ESTRO volume? The two patients with marginal misses outside the volume were both ER−/HER2− and ypN+ patients who had a poor response (non-pCR) to neoadjuvant chemotherapy, and subsequently progressed to widespread distant metastases. In other words, this should be interpreted as a consequence of poor underlying tumor biology rather than a flaw in the ESTRO volume definition itself.
Given that this validation was conducted prospectively within a large-scale phase III RCT, and directly by the Offersen group that established the ESTRO guidelines, I believe the level of evidence is exceptionally high. Put another way, there are fewer and fewer reasons not to adopt the ESTRO guidelines going forward. |
|
|
✅ How OncoStudio Approaches Contouring
Oncosoft's auto-contouring software, OncoStudio, also operates on the principle of strictly adhering to the ESTRO guidelines as closely as possible. When I provided clinical consultation for data curation, we carefully integrated several practical considerations for real-world clinical workflows. For example, while ESTRO classifies interpectoral (Rotter) nodes as a separate structure, we included them within Level II for routine clinical convenience. We also chose to provide the RTOG-standard SCL alongside Level IV (ESTRO SCL), allowing users to select the appropriate option based on their specific clinical scenarios. Regarding Level III, since the auto-contours tend to be drawn slightly more cranially than the guidelines suggest, users can make minor adjustments to trim any unnecessary areas. Furthermore, with the recent publication of the ESTRO contouring guidelines for breast reconstruction patients, Oncosoft is currently retraining its model by adding labels for implant patients, which we expect to roll out in the near future.
I hope that OncoStudio will contribute to a virtuous cycle where high-quality guidelines are supported by robust evidence and seamlessly integrated into the tools clinicians use every day.
|
|
|
(This column was drafted with the assistance of Claude AI and subsequently reviewed and finalized by the author.) |
|
|
|