- OncoStudio Completes U.S. USPTO Trademark Registration
- OncoStudio’s Impact Confirmed in Gil Medical Center Clinical Research
- KHC 2026
- Novartis RLT Summit
- KSMP 2026: Technical Exchange through 'OncoFlow'
- ITEM 2026: Solidifying Brand Presence and Strengthening Partnerships in Japan
- [Upcoming Event]
- KOSRO Spring Meeting (Gangneung) – May 8
- [Column]
- News in RadOnc
- CEO Insight
|
|
|
❶ OncoStudio Completes U.S. USPTO Trademark Registration |
|
|
OncoStudio, Oncosoft’s flagship AI solution, has officially completed its trademark registration with the United States Patent and Trademark Office (USPTO). This registration marks a significant milestone, securing exclusive brand rights in the U.S.—the world’s largest healthcare market. It establishes a robust legal foundation for Oncosoft's ongoing localization and commercialization efforts in North America. Leveraging this enhanced brand protection, Oncosoft plans to aggressively pursue global partnerships and marketing activities to expand its international market presence. |
|
|
❷ OncoStudio’s Impact Confirmed in Gil Medical Center Clinical Research |
|
|
A recent study published in the journal Radiation Oncology by the research team at Gachon University Gil Medical Center highlights OncoStudio as a key tool for enhancing research efficiency. Researchers utilized OncoStudio’s auto-contouring feature for organ segmentation to ensure high accuracy and data consistency. The study noted that the AI-driven process maintained precision even in complex anatomical structures, significantly improving workflow efficiency. This case reinforces OncoStudio’s reputation as a trusted solution for enhancing objectivity and reliability in demanding clinical environments. |
|
|
❸ KHC 2026: Insights on the Paradigm Shift in Particle Therapy |
|
|
At the 15th Korea Healthcare Congress (KHC 2026) held on April 10, CEO Jin Seung Kim delivered a presentation titled "The Present and Future of Advanced Accelerator-Based Particle Therapy." Dr. Kim explained that as radiation therapy evolves from wave-based to mass-bearing particle therapy, the ability to utilize the "Bragg Peak" has become a core competency. He emphasized that in an era of 2.73 million cancer survivors, integrating Oncosoft’s AI technology with advanced facilities like heavy-ion accelerators is essential. This integration is key to optimizing treatment precision and shaping the future of national cancer care. |
|
|
❹ Novartis RLT Summit: Strategies for Workflow Efficiency |
|
|
On April 24, CEO Jin Seung Kim spoke at the Novartis RLT (Radiopharmaceutical Therapy) Summit regarding integrated platforms for workflow and patient safety. Dr. Kim highlighted the limitations of current fixed-dose administration and stressed the importance of individualized dosimetry that accounts for varying drug absorption rates among patients. Oncosoft aims to apply its expertise in AI contouring and dose calculation to the RLT field. The company is developing an intelligent workflow platform designed to ensure optimal dosing and enhanced patient safety. |
|
|
❶ KSMP 2026: Technical Exchange through 'OncoFlow' |
|
|
Oncosoft participated in the Korean Society of Medical Physics (KSMP) 2026 Spring Conference on April 10 to engage with domestic medical physics experts. In addition to demonstrating the AI-based contouring solution OncoStudio, the company focused on introducing its new "OncoFlow" platform. Through in-depth discussions, Oncosoft gathered practical feedback on how OncoFlow can improve clinical workflow efficiency and service scalability. These insights will serve as a vital foundation for future product enhancements and clinical updates. |
|
|
❶ ITEM 2026: Solidifying Brand Presence and Strengthening Partnerships in Japan |
|
|
From April 17 to 19, Oncosoft showcased its technological prowess at ITEM 2026 in Yokohama, Japan. Following its successful entry into the Japanese market, Oncosoft has secured purchase commitments from several major medical centers and is expanding trust through successful demo operations at approximately 50 sites. Moving forward, Oncosoft will collaborate closely with its local partner, Anzai, to position its solutions as key strategic additions to their portfolio. This alignment is intended to strengthen the supply chain and market response across the Asia-Pacific region. |
|
|
❶ KOSRO Spring Meeting (Gangneung) – May 8
|
|
|
Oncosoft will participate in the Korean Society for Radiation Oncology (KOSRO) Spring Meeting in Gangneung on May 8. We look forward to showcasing our latest AI technological advancements and strengthening our network with radiation oncology specialists and industry stakeholders. By presenting a vision where AI enhances treatment accuracy and reduces the burden on medical professionals, we remain dedicated to leading the innovation of radiation therapy in Korea. |
|
|
- Date: May 8, 2026
- Venue: Skybay Hotel Gyeongpo, Gangneung
|
|
|
✅ Why Repeat SABR?
A 5-Year Journey of 17 Lesions in a Single Patient
"How would you feel about treating a single patient with SABR 17 times across 8 sessions over a 5-year period? (Ashraf S, …, David S. Front Oncol 2026;16:1641876)
|
|
|
In my practice, I have several patients following a similar trajectory. One patient maintained the same systemic therapy for five years by using SABR to "push down" individual lesions whenever they cropped up, allowing them to maintain an active daily life through over 10 repeated treatments. Recently, when this patient transferred to another hospital to participate in a clinical trial, I received a phone call from a medical oncologist there.
"I was stunned looking at the medical records. I didn't know so many radiation treatments were possible, nor did I expect the patient to be in such excellent shape—especially while staying on the same drug for so long. Could I refer some of my own patients who might need this kind of approach?"
While this might be considered an "extreme version" of oligoprogression, similar cases are increasingly surfacing. At a recent SABR symposium, a case report from Dr. Steven David’s group at the Peter MacCallum Cancer Centre in Australia garnered significant attention. Today, I would like to walk through that journey.
|
|
|
✅ 5 Years and the Strategy of a Single Patient
|
|
|
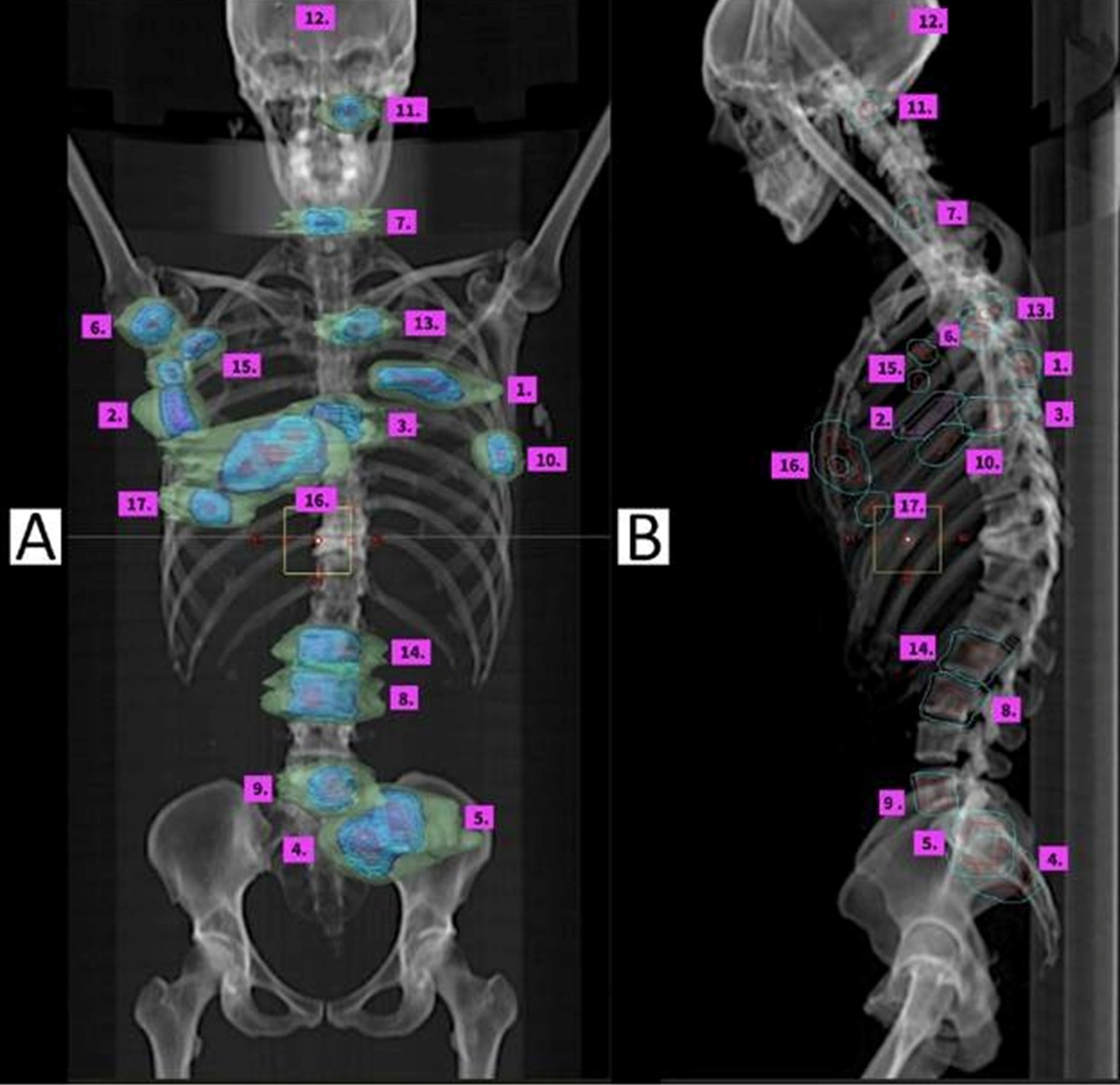
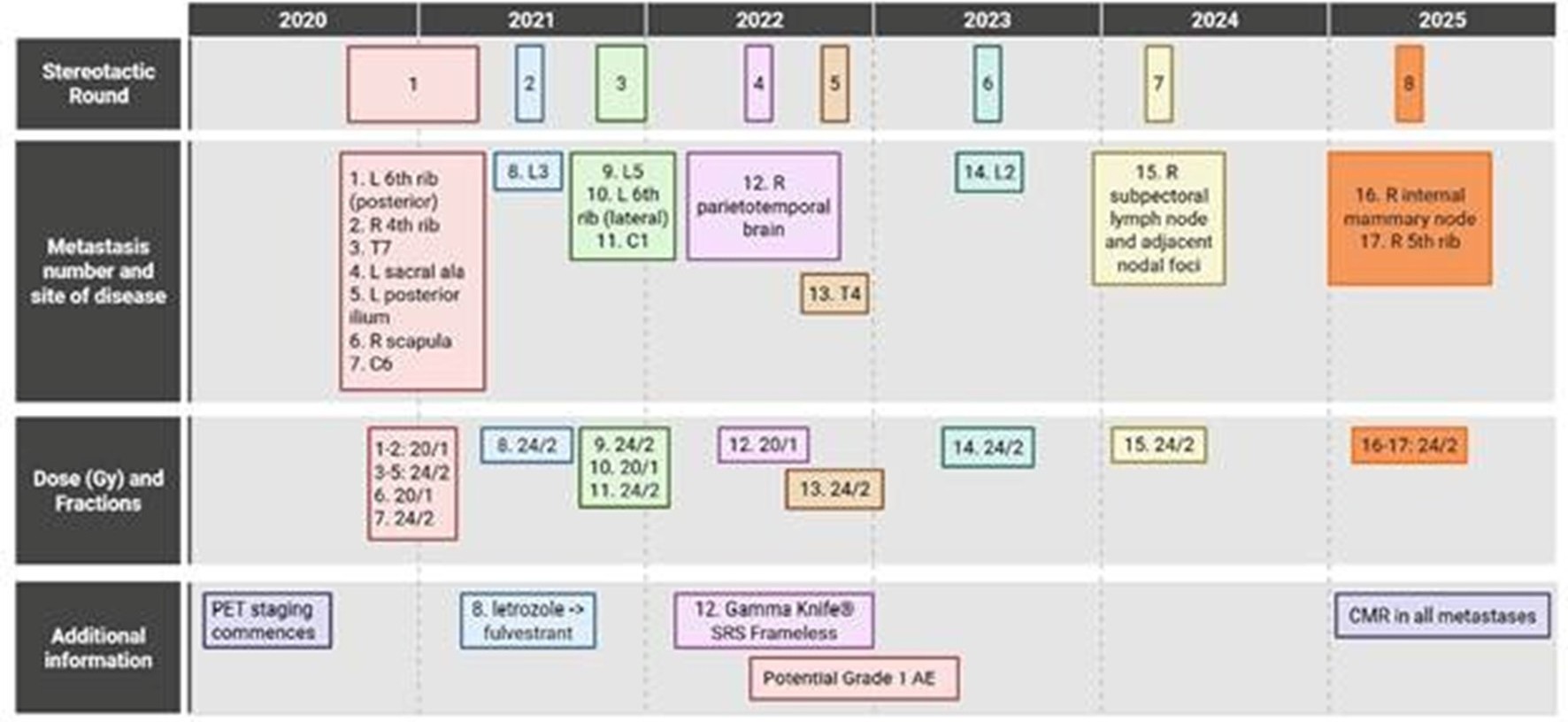
The clinical record tracks a 5-year trajectory across the skull (Gamma Knife for brain metastases), ribs, thoracic spine, lumbar spine, sacrum, scapula, and lymph nodes. Seventeen distinct locations were treated with SABR. Remarkably, the patient maintained an ECOG 0 status throughout, raising two children and exercising regularly. At the final follow-up, all lesions showed a complete metabolic response, with zero recurrences at previous treatment sites. |
|
|
✅ 35-Year-Old, De Novo Metastatic Breast Cancer
The patient was diagnosed in 2017 at age 35 with ER+/PR+/HER2+ de novo metastatic breast cancer. Following induction with paclitaxel, trastuzumab, pertuzumab, and denosumab, she was stabilized on maintenance therapy. In late 2020, as PET-CT became the primary staging modality, her journey of serial SABR began:
|
|
|
- Round 1 (2020): SABR to 7 lesions, including the left 6th rib.
- Round 2 (2021): L3 oligoprogression. Endocrine therapy switched from letrozole to fulvestrant; this regimen was then maintained for the next 5 years.
- Round 3 (2021): 3 lesions (L5, left 6th rib, C1).
- Round 4 (2022): First non-bone lesion (brain metastasis), treated with Gamma Knife (20Gy/1).
- Round 5 (2022): T4.
- Round 6 (2023): L2.
- Round 7 (2024): Right subpectoral LN. SABR chosen to delay the toxicity of the next systemic option (Trastuzumab deruxtecan, T-DXd).
- Round 8 (2025): Right internal mammary node + 5th rib. Again, SABR used to defer T-DXd.
The core strategy was delaying a change in systemic therapy at every round. The result? 5 years, 17 lesions, 8 interventions. The patient was an active participant in shared decision-making, consistently expressing a preference to maintain her current effective medication for as long as possible. |
|
|
✅ Managing the Re-irradiation Space
As a clinician, I want to highlight the planning strategy for new lesions adjacent to previously treated areas. |
|
|
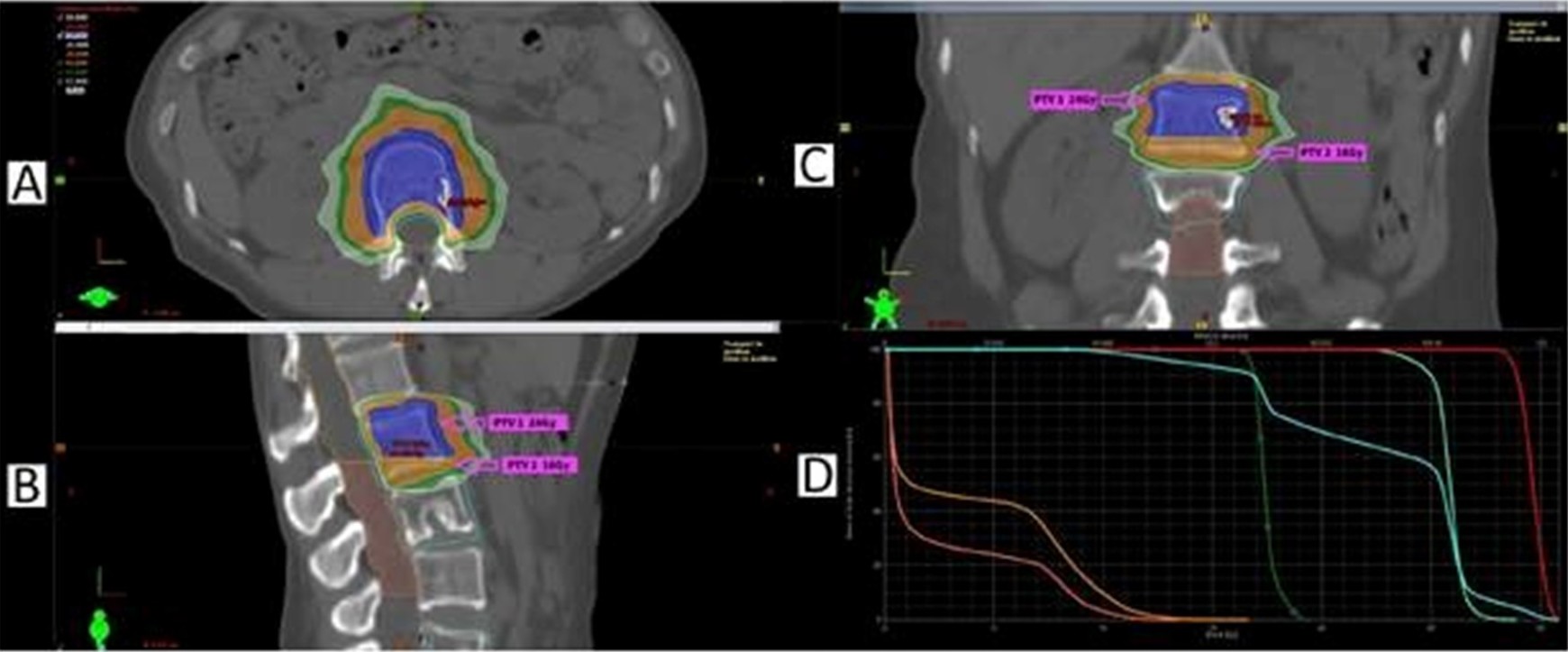
Figure 3. Round 6 L2 SABR plan. Since the adjacent L3 region had previously received SABR in Round 2, the PTV was divided into two dose levels (24 Gy / 16 Gy), and the spinal canal dose was separated into superior (14 Gy) and inferior (12 Gy) regions. |
|
|
Round 6 (L2): This was adjacent to the L3 treated in Round 2. To respect spinal cord constraints, the PTV was split into two sub-PTVs (24Gy and 16Gy), and the spinal canal was segmented into superior (14Gy) and inferior (12Gy) doses. The cumulative BED (α/β=3) in the overlapping region was kept to a safe 178.67 Gy. |
|
|
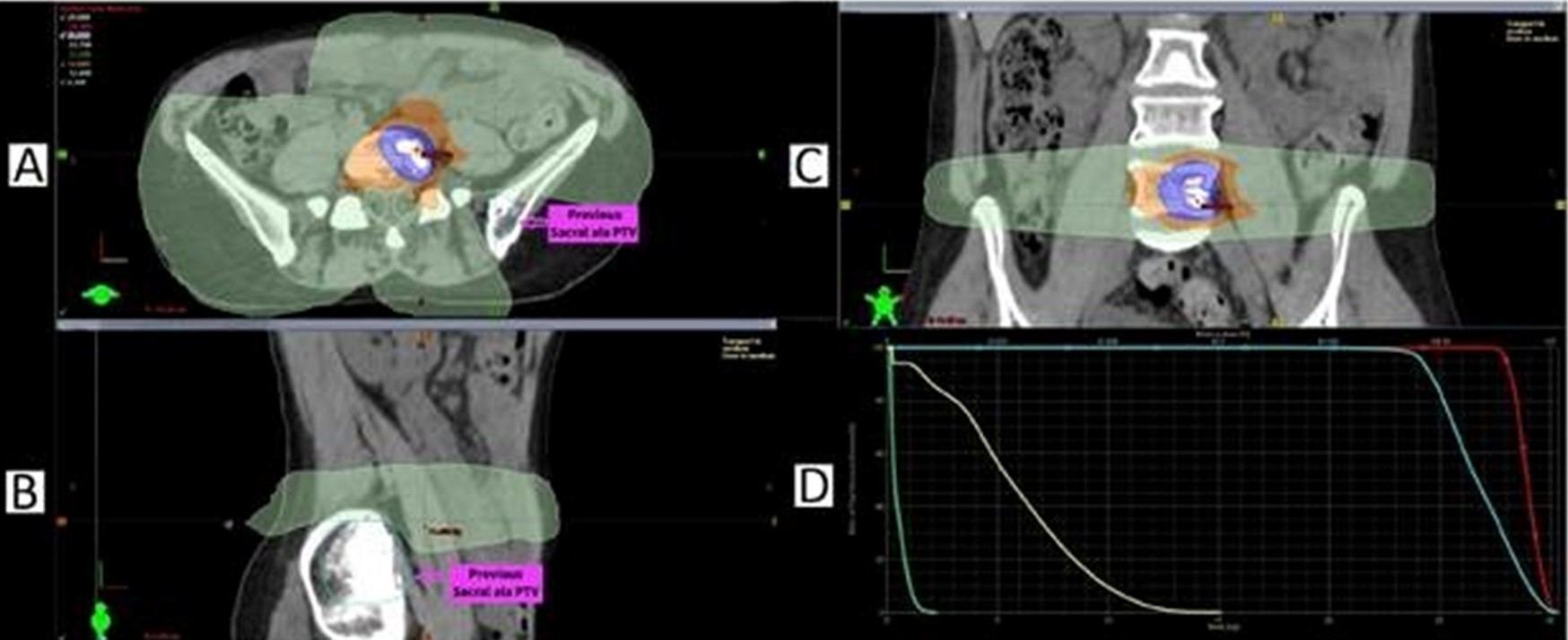
Figure 4. Round 3 L5 SABR plan. The left sacral ala treated in Round 1 was almost completely spared, and the maximum dose to the previous PTV was kept below 2.5 Gy.
|
|
|
Round 3 (L5): By leveraging the sharp dose fall-off of SABR, the plan for L5 (24Gy/2) almost entirely avoided the previously treated left sacral ala from Round 1, keeping the prior PTV max dose under 2.5 Gy. |
|
|
✅ This Is Not Actually New
While 17 sites is an extreme case, the pattern of "Repeated SABR" is more common than we realize. Long-term follow-up from the SABR-COMET trial showed that about 30% of 5-year survivors received additional SABR for new metastases. In our study of 1,143 colorectal lung metastases (Lee BM et al. Ann Surg 2023), 33% received an average of 2.4 additional metastasis-directed treatments, with overall survival rates nearly identical to those who never recurred.
The challenge lies in how we measure this effect in clinical trials. RECIST v1.1-based PFS stops the clock at the first progression event. It fails to capture the time gained by delaying a change in systemic therapy through additional SABR. This mismatch between endpoints and "Strategic RT" is likely why trials like NRG-BR002 and NRG-LU002 failed to show survival benefits despite using PFS as a primary endpoint.
I addressed this in a recent editorial (Cancer Letters 2025), arguing that the value of Serial Strategic RT is better captured by endpoints like PFS2, mPFS, or TTNT (Time to Next Treatment). Dr. David’s patient is the perfect clinical illustration: under traditional RECIST PFS, her "benefit" would have vanished the moment L3 progressed after Round 1. |
|
|
✅ The Path Blazed by Brain SRS
We have seen this shift before. I recall the early 2010s during my residency when repeating Gamma Knife for brain metastases was met with skepticism. "Why not just do WBRT?" was the common refrain. Today, WBRT is fading, and the indications for brain SRS are expanding because evidence proved we could preserve cognitive function without compromising oncologic outcomes.
I believe extracranial SABR is on a similar path. The current "strangeness" of treating a Stage IV patient eight times will eventually become a standard option. While we still need more high-level evidence and better patient selection tools (like ctDNA), the trend is unmistakable.
The tools we are building at Oncosoft are inextricably linked to this direction. Whether it is streamlining plan efficiency, tracking cumulative doses, or evaluating re-irradiation safety, we aim to be a dependable partner for clinicians in this new era of Serial SABR. |
|
|
(This column was refined in collaboration with Claude AI based on my specific clinical experiences and selected literature. All clinical insights and final revisions were conducted by the author.) |
|
|
📍Generative AI, Medicine, and Us
– Where are Medical Physics and Radiation Oncology Headed?
"What will happen to my job in the age of AI?"
This was a question recently posed by one of our data team members. From the shock of AlphaGo in 2016 to 2026, where Generative AI—technologies like ChatGPT, Gemini, and Claude—is seamlessly embedded in everything from coding to clinical insights, this concern is no longer a distant future. It is our reality.
We are now witnessing complex code being written in seconds and tasks that once took days being completed with startling quality. In this whirlwind of change, some roles are vanishing, and certain efforts no longer hold the same value they once did. The medical field is no exception. Generative AI is creating a shift on a completely different dimension, offering outputs that closely resemble clinical judgment. While this significantly boosts efficiency, it forces us to confront a fundamental question:
"Are we still thinking for ourselves?"
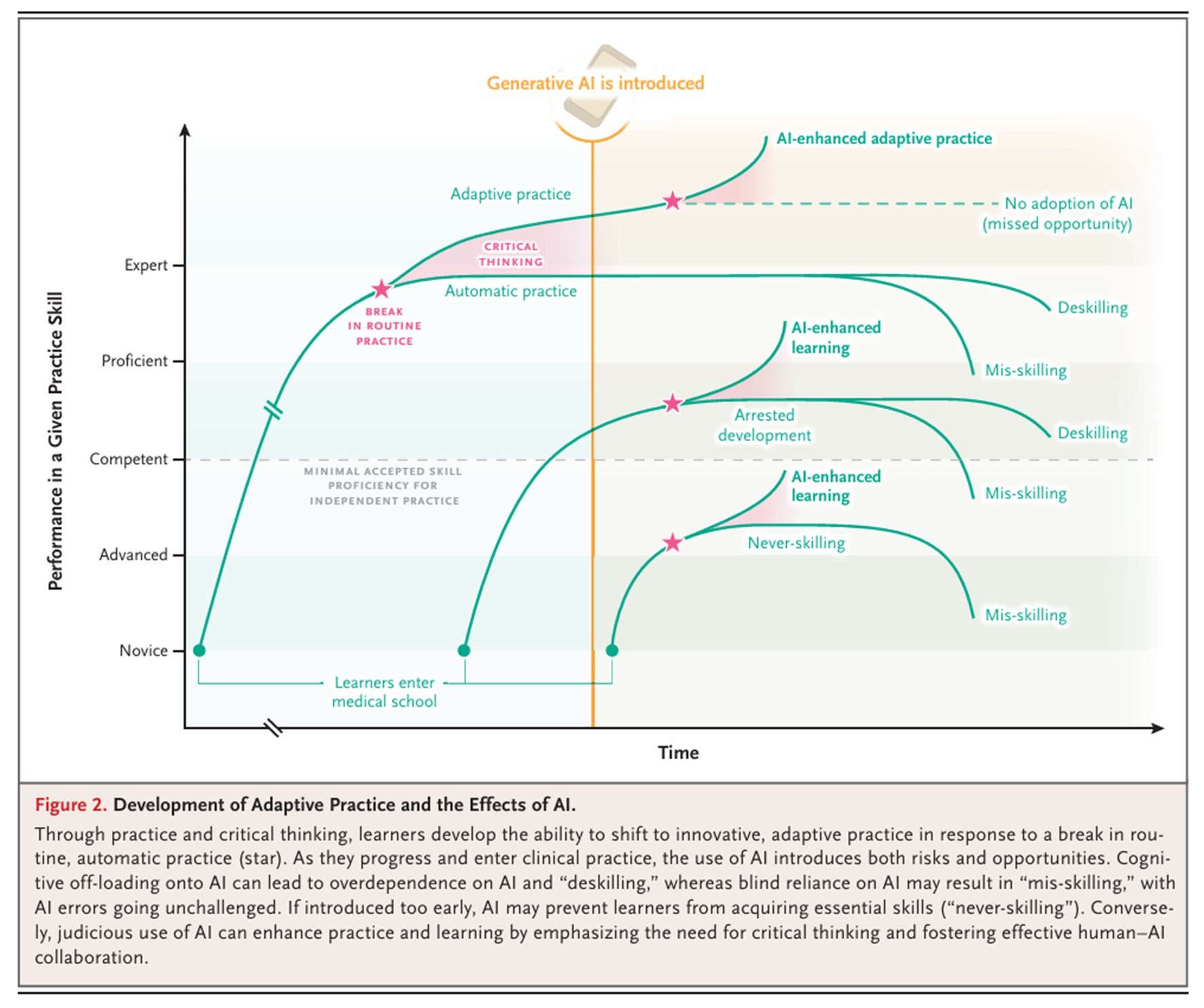
A recent article in the New England Journal of Medicine (2025;393:786-97), "Educational Strategies for Clinical Supervision of Artificial Intelligence Use," provides a meaningful perspective on this.
|
|
|
We have traditionally grown into "Adaptive Experts" through a rigorous process of repetition and experience. However, the advent of Generative AI is quietly but deeply altering this path of growth. If we lean too heavily on convenience and let go of the process of thinking, we risk falling into the traps of de-skilling, where we lose our innate professional abilities; mis-skilling, where we absorb and normalize flawed AI outputs; or never-skilling, where we build results on a foundation that never had the chance to solidify.
Ultimately, AI must not be an entity that thinks instead of us, but a tool that makes our thinking deeper. These changes are already manifesting in clinical practice, and within this shift, the roles of medical professionals are not disappearing but are being redefined more clearly than ever. The medical physicist becomes the final gatekeeper ensuring that AI results are physically valid and safe, the dosimetrist becomes the strategist who finds the optimal treatment plan among a sea of options, and the radiation oncologist stands at the center, integrating all information to make the most meaningful decisions for the patient.
The essence of the change we face is not about technology, but about our way of thinking. True competitiveness in the AI era does not depend on the volume of knowledge, but on how we understand, doubt, and select that knowledge. We must no longer be mere users of AI; we must be those who understand, question, and verify it to the very end.
This reflection continues at Oncosoft. As we develop AI contouring and define the goals for OncoPlan and OncoFlow, we are contemplating not just technical perfection, but the professional philosophy these tools should embody.
It is not an easy path, but I believe that as long as we do not stop asking questions, we will not lose our way. If you join us in this reflection and continue to question with us, that in itself will be a great source of strength.
Thank you.
|
|
|
|